Dengue is a mosquito-borne viral illness caused by the dengue virus, transmitted by the Aedes mosquito.
- One of the most common causes of “undifferentiated tropical fevers”.
- It is associated with higher morbidity and mortality especially in children. The risk of death is fourfold higher in children younger than 15 years of age.
Case Definition
- Dengue fever: Acute febrile illness (2-7 days) with one or more of the following: Headache, retrorbital pain, myalgia, arthralgia, rash, hemorrhagic manifestations. OR, non-ELISA based nonstructural glycoprotein-1 (NS-1) antigen/IgM tested positive.
- Severe Dengue: Consider if the patient is from an area of dengue risk presenting with fever of 2–7 days plus any of the following features:
- Evidence of plasma leakage
- High or progressively rising haematocrit
- Pleural effusions or ascites
- Circulatory compromise or shock (tachycardia, cold and clammy extremities, capillary refill time >3 sec, weak or undetectable pulse, narrow pulse pressure or, in late shock, unrecordable blood pressure).
- Significant bleeding
- Altered level of consciousness (lethargy or restlessness, coma, convulsions)
- Severe gastrointestinal involvement (persistent vomiting, increasing or intense abdominal pain, jaundice)
- Severe organ impairment (acute liver failure (AST or ALT >1000), acute renal failure, encephalopathy or encephalitis, ARDS or other unusual manifestations.)
- Evidence of plasma leakage
| Warning Signs in Dengue Fever | -Abdominal pain or tenderness • Persistent vomiting • Clinical fluid accumulation • Mucosal bleed • Lethargy, restlessness • Liver enlargement >2 cm • Laboratory: increase in HCT concurrent with rapid decrease in platelet count |
Clinical Course of Dengue
| Febrile phase (2-5 days) | Patient remain febrile throughout this period, fever is biphasic |
| Critical phase (after 3-4 days of onset of fever) | -Plasma leakage and hemoconcentration starts -May develop hypotensive shock and progressive organ dysfunction |
| Convalescent phase (Start after 6–7 days of fever and lasts for 2–3 days) | -ECF lost due to capillary leakage returns to circularity system – Clinical status improves |
History and Examination
Children living or traveling in endemic areas, recent mosquito bites
Symptoms
- High fever (40°C/104°F)
- Headache
- Retro-orbital pain
- Myalgia
- Arthralgia
- Nausea and vomiting
- Rash
Signs
- Petechiae, ecchymoses, or purpura
- Hepatomegaly
- Positive tourniquet test
Differential Diagnosis (D/D) & Complications
D/D
- Malaria (cyclical fever, anemia, splenomegaly)
- Leptospirosis (jaundice, renal dysfunction, conjunctival suffusion)
- Scrub typhus (eschar, lymphadenopathy)
- Typhoid
- Bacterial sepsis
Complications
- Dengue hemorrhagic fever (DHF)
- Dengue shock syndrome (DSS)
- Multi-organ failure
- Hypo/Hyperglycemia
- Electrolyte abnormalities
- Nosocomial/Co-infection
- Metabolic Acidosis
Investigation
- Investigation of choice
- NS1 antigen detection (Day 1-5 of illness)
- IgM
- Appears after day 5
- Can be detected up to a year so lower sensitivity and specificity
- IgG
- Detected after 1-2 weeks and persist for life
- Complete blood count (CBC) with platelet count and peripheral smear
- Leukopenia with lyphocytoses
- Leukocytosis in recovery phase precedes rise in platelets count
- Platelets declines in critical phase, rise in platelets in clinical recovery
- Hematocrit
- Normal in uncomplicated case, high when capillary refill starts
- Clinical significant only when 20% rise over the baseline
- Monitoring it helps in titrating fluid therapy
- Liver and renal function tests
- Mild elevated; AST>ALT
- Low albumin in sever disease
- Coagulation test
- Raised PT/INR, and aPTT
- RFT
- Increased creatinine, proteinuria, and hyponatremia
- Blood grouping and Cross Matching
- ABG:
- Metabolic acidosis and elevated lactate levels seen in shock
- Chest x-ray
Admission Criteria
- Severe dengue (DHF or DSS)
- Platelet count < 100,000 /cu.mm or rapidly decreasing trend
- Hematocrit is rising trend.
- Children with warning signs (persistent vomiting, abdominal pain, rapid decrease in platelet count)
- Poor oral intake, dehydration
- Living far from a health facility without reliable means of transport
Indications for Pediatric Intensive Care Unit Admission
- Severe plasma leakage with hypoperfusion and hypotension
- Fluid accumulation with respiratory distress
- Severe bleeding
- Severe organ impairment:
- Myocardial dysfunction
- Acute kidney injury
- CNS dysfunction (altered consciousness and seizures)
- Hepatic dysfunction (ALT/AST >1,000 IU)
- HLH
Management
Case classification
| Mild (Outpatient management) | Moderate (Inpatient management) | Severe (ICU management) |
| -Fever for 2-7 days -Associated features nausea, vomiting, rash, headache, retro-orbital pain, myalgia, arthralgia, and leukopenia | Dengue with high-risk comorbid condition -Infants -Using immunosuppressive drugs or immunocompromised status -Any coagulation disorder -Dengue with warning signs |
Medical Management
# Out Patient Management
- Give Paracetamol for fever (Do not prescribe Flexon as it has Ibuprofen like acetylsalicylic acid (aspirin), and like other non-steroidal anti-inflammatory agents are contraindicated in dengue fever because they can aggravate gastritis or bleeding)
- Adequate rest and fluid intake (Milk, fruit juice, electrolyte solution (ORS) and barley/rice water)
- Tepid sponging
- Antibiotics are not necessary
Tell patient party to observe for the following Danger signs and report immediately for hospital admission:
- Bleeding (Red spots or patches on the skin; bleeding from nose or gums; vomiting blood; black-coloured stools; heavy menstruation/vaginal bleeding)
- Frequent vomiting
- Severe abdominal pain
- Drowsiness, mental confusion or seizures
- Pale, cold or clammy hands and feet
- Difficulty in breathing
# In patient management
- Obtain baseline CBC, monitor intake and output, monitor vital signs 4 hourly or frequently
- Good oral fluid intake
- Encourage oral fluid intake
- Observe for warning sign
- Do symptomatic treatment
- Poor oral fluid intake
- Check hematocrit (HCT). Obtain baseline hematocrit before starting fluid.
- Give IV Isotonic crystalloid solution (NS,RL) in step wise manner
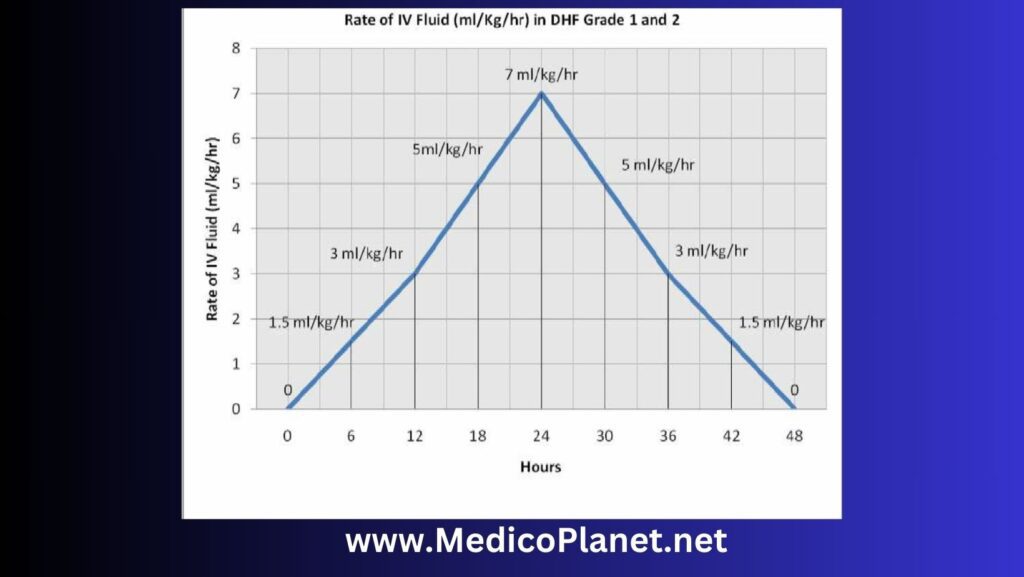
- Start with 5 ml/kg/hour for 1–2 hours, then reduce by 2ml/kg/hour every 2 hours till 2ml/kg/hr provided there is clinical improvement and haematocrit is appropriately improving. IV fluids are usually required for 1-2 days.
- 5-7 ml/kg/hr for 1-2 hours
- 3-5 ml/kg/hr for 2-4 hours
- Recheck HCT and reassess clinical status
- Reassess the clinical status and repeat the haematocrit after 2 hours: If the haematocrit remains the same, continue with the same rate for another 2–4 hours and reassess. If the vital signs/haematocrit is worsening increase the fluid rate.
- Clinically stable with no or minimal change in HCT
- Continue fluid 2-3 ml/kg/hr for 2-4 hours
- Decrease the fluid as patient become clinically stable, with adequate fluid intake and output, HCT decrease to baseline
- Worsening vital signs or increasing HCT
- Increase IV fluid to 5-10 ml/kg/hour for 1-2 hours
- Recheck the status and HCT
- If improving, gradually decrease the fluid
- If not, follow ICU management
# Severe (ICU management)
Inpatient management of dengue patients with dengue shock
- Dengue shock syndrome (poor peripheral perfusion, hypotension, BP not recordable)
- Give oxygen via facemask
- Immediate rapid volume replacement
- 10-20 ml/kg NS or RL over 30 minutes
- 10ml/kg for compensated shock
- 20ml/kg for hypotension
- Improvement (Decrease HCT, Stable BP and HR, Urine output: 0.5 to 1 ml/kg/hr)
- Start IV therapy with NS or RL
- Titrate the flow from
- 10-7 ml/kg/hr for 2-4 hours
- 5-3 ml/kg/hr for 2-4 hours
- 3-1.5 ml/kg/hr for 2-4 hours
- Titrate the flow from
- If patient improve, discontinue fluid after 24 to 48 hours
- Total fluid therapy usually 24-48 hrs, titrated to adequate urine output. Give the minimum intravenous fluid volume required to maintain good perfusion and urine output of about 0.5 ml/kg/hr. Stop fluid when urine output is adequate, patient is stable, adequate oral intake and or hematocrit decreasing below the baseline value.
- Cautious fluid resuscitation is very important to avoid overloading.
- When “capillary leak” progress, children have a tendency to develop “fluid creep” and worsening respiratory status.
- Fluid resuscitation at the cost of respiratory worsening may not culminate in good outcome.
- Start IV therapy with NS or RL
- No improvement (Rise in HCT or HR, Pulse pressure falls below 20 mm Hg, urine output falls)
- Repeat second bolus: 10-20 ml/kg of crystalloid (preferably colloid: Dextran 40) over 30 minutes
- Improvement or rise in HCT (>45%)
- Repeat third bolus: 10-20 ml/kg of crystalloid (preferably colloid) over one hours
- No improvement, HCT falls, or suspected bleeding
- Blood transfusion
- 10ml/kg whole blood / 5ml/kg PRBC
- No improvement
- Look for myocardial dysfunction (ECG), correct acidosis, hypoglycemia, and electrolyte abnormalities
- Echocardiograpy
- IV Inotropes with fluid replacement therapy
- Blood transfusion
- Improvement or rise in HCT (>45%)
- Repeat second bolus: 10-20 ml/kg of crystalloid (preferably colloid: Dextran 40) over 30 minutes
- 10-20 ml/kg NS or RL over 30 minutes
Indications for platelet transfusion
- Shock, acidosis with rapidly declining platelets (greatest risk of DIC)
- Significant mucosal bleeds (harbinger of intracranial hemorrhage)
- Platelet count < 20,000 cu mm in the acute phase
- Need for invasive procedures such as central lines maintain platelet count > 50,000 cu mm
- A low platelet count is less significant after recovery from shock and may not need to be transfused.
Treatment of Fluid overload
- Fluid overload with large pleural effusions and ascites is a common cause of acute respiratory distress and failure in severe dengue.
- Other causes of respiratory distress include acute pulmonary oedema, severe metabolic acidosis from severe shock, and Acute Respiratory Distress Syndrome (ARDS).
- Do the chest x-ray if find sign of fluid overload
- Rx:
- Oxygen therapy/ventilation if indicated should be given immediately.
- Stopping intravenous fluid therapy during the recovery phase will allow fluid in the pleural and peritoneal cavities to return to the intravascular compartment resulting ion dieresis.
- Give diuretics if necessary: Oral or intravenous furosemide 0.1–0.5 mg/kg/dose once or twice daily, or a continuous infusion of furosemide 0.1 mg/kg/hour.
Criteria for discharge
- Absence of fever for at least 24 hrs without any use of antipyretic
- Return of appetite
- Clinical improvement
- Good urine output
- Stable haematocrit
- Normal organ function workup results
- No respiratory distress from pleural effusion and ascites
- No other complication
Advices
- Educate the family on mosquito prevention measures (insect repellent, protective clothing, mosquito nets)
- Encourage oral rehydration
Referral
- All patients with Warning signs and signs of Severe dengue.
- Patients not clinically responding to therapy in situation.
- Patients with serious co-morbid conditions
- Platelet counts < 50,000/cu.mm with a decreasing trend.
Follow up
- Schedule a follow-up visit within 7-10 days after recovery
- Monitor for any complications or signs of post-dengue fatigue
Additional Points
Fluid choice in Dengue
- Normal saline\Ringer’s lactate
- In severe/refractory shock, colloids such as Plasma , plasma substitutes (6% hetastarch/dextran/ / 5% albumin /) may be preferred
- Fresh whole blood or packed red blood cells may be needed for persistent shock despite restoration of fluid volume and a fall in haematocrit, suggesting the possibility of occult blood loss.
- Rapidly administered dextrose containing solution when used for resuscitation may result in hyperglycemia and osmotic diuresis, delaying correction of hypovolaemia. Secondly, dextrose is rapidly metabolized resulting in a hypotonic solution that is inappropriate for shock correction.
Recognition of Shock
- Tachycardia , Low pulse volume
- Capillary Refill time > 2 sec
- Narrow pulse pressure
- Blood pressure less than the 3rd centile for age
- Cold clammy peripheries
- Altered sensorium
- Poor urine output [ <0.5ml/kg/hr consistently ]
- Tachypnoea
- Metabolic acidosis
Choice of Vasoactive agents/ post resuscitation fluid removal
- Shock with low BP for age: Dopamine 10mcg/kg/min OR Noradrenaline/adrenaline 0.1-0.2mcg/kg/min
- Shock with normal BP for age: Dobutamine 5-10mcg/kg/min
- Shock with diastolic dysfunction on echo: Milrinone 0.25-0.75mcg/kg/min (no
- loading dose)
- Predominant pulmonary edema, haemodynamics stable : Nitroglycerine 1-3mcg/kg/min, furosemide infusion 3- 5mg/kg/day, titrate to urine output of 3-5 ml/kg/hr. Cease infusion and infuse fluid if hypoperfusion occurs.
- Pulmonary edema, fluid overload, haemodynamics unstable: Ventilation vital (high risk of mortality), can consider peritoneal dialysis if 24 hour experienced nursing and medical staff available in PICU
# Important points
- Serial haematocrit measurement (if not bleeding), and urine output provide the most objective guides to fluid replacement and prevention of fluid overload.
- Aim for ≈ 20% fall in haematocrit and adjust fluid rate downwards to avoid overload
- Aim for minimal acceptable urine output (0.5-1ml/kg/hr)
- A urine output > 3 ml /kg /hour indicates Hypervolaemia
- Fluid replacements are dynamic hence require continuous reassessments.
- No dextrose containing fluid should be used for fluid resuscitation, Separate maintenance fluids are usually not required. Glucose/potassium may need to be given separately. Start enteral feeds early.
- All invasive procedures must be performed by most experienced person. If possible, aim for platelets > 50,000/cu mm prior to central line insertion.
- Profuse bleeds may necessitate transfusion of platelets and FFP regardless of lab values: conversely, low platelet counts in the recovering, stable patient may not be an indication for transfusions
References
1. World Health Organization. Dengue: Guidelines for Diagnosis, Treatment, Prevention, and Control. Geneva: World Health Organization; 2009.
2. Guzman MG, Harris E. Dengue. Lancet. 2015;385(9966):453-465.
3. Simmons CP, Farrar JJ, Nguyen V, Wills B. Dengue. N Engl J Med. 2012;366(15):1423-1432.