Tracheoesophageal fistula (TEF) is a congenital anomaly characterized by an abnormal connection between the trachea and the esophagus.
- Often occurs in conjunction with esophageal atresia.
- Associated with congenital heart disease (Patent foramen ovale, PDA, VSD)
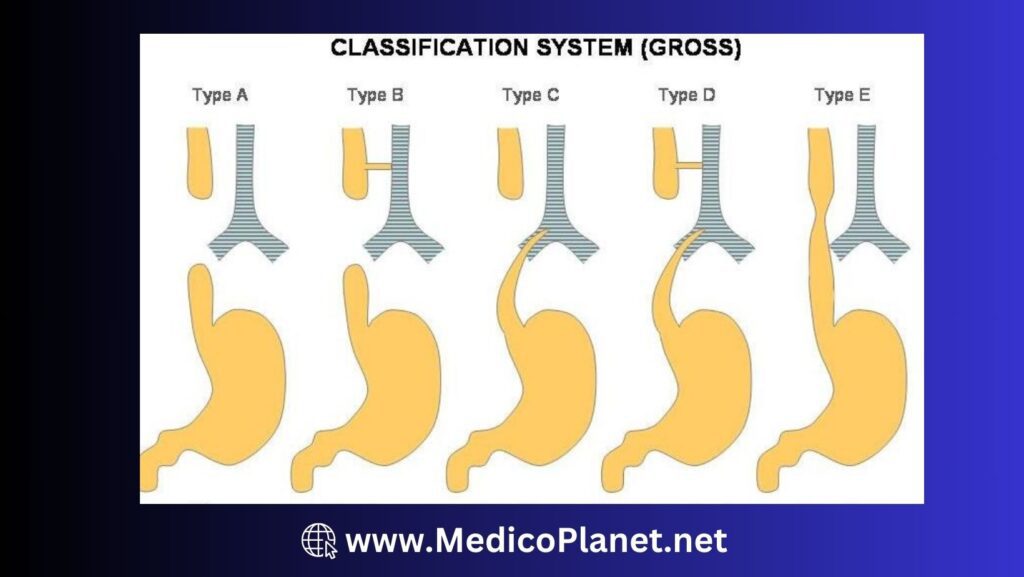
| Type A | 7% | Esophageal atresia only, no connection between esophagus and trachea |
| Type B | 2% | Proximal esophagus connect with trachea |
| Type C | 86% | Distal esophagus connect with trachea |
| Type D | 1% | Both proximal and distal end of esophagus connect with trachea separately |
| Type E | 4% | Both proximal and distal end of esophagus connect with trachea and there is connection between both ends |
History and Examination
Risk factors: Maternal polyhydramnios, family history, chromosomal abnormalities, VACTERL association
Often detected in the prenatal period or shortly after birth
| Symptoms | Signs |
| Excessive frothing from mouth Coughing and choking while attempting to swallow Cyanosis during feeding Respiratory distress | Frothy secretions and saliva in the mouth and nose Abdominal distension Inability to pass a nasogastric tube into the stomach |
Differential diagnosis (D/D) & Complication
D/D:
• Choanal atresia (Unilateral or bilateral nasal obstruction, no feeding issues)
• Laryngeal cleft (Recurrent aspiration, no esophageal issues)
• Congenital diaphragmatic hernia (Respiratory distress, scaphoid abdomen)
Complications:
• Aspiration pneumonia due to reflux of gastric contents through the fistula.
• Malnutrition
• Respiratory complications
• Gastroesophageal reflux
Investigation
Prenatal ultrasound (for polyhydramnios)
X-ray Chest + Abdomen: Before doing x-ray, insert the NG tube. In TEF, there will be coiling of NG tube.

Admission Criteria
Infants with confirmed or suspected TEF require immediate admission for surgical evaluation and management
Management
Emergency management
- Secure Airway, elevate head, do suctioning of secretion
- IV line access and start fluid therapy
Medical– No medical management required.
Surgery
- Indication: Confirmed diagnosis of TEF
- Procedure: Primary repair of the TEF and esophageal atresia
After initial management refer patient to pediatric surgeon for surgical management.
References
- Choudhury, S. R., & Ashcraft, K. W. (2016). Esophageal atresia and tracheoesophageal fistula. In Holcomb and Ashcraft’s Pediatric Surgery (6th ed., pp. 377-394). Elsevier.
- Bairdain, S., & Hamilton, T. E. (2018). Surgical management of esophageal atresia and tracheoesophageal fistula. Seminars in Pediatric Surgery, 27(2), 92-98.
- Rothenberg, S. S. (2012). The first decade’s experience with thoracoscopic repair of esophageal atresia in infants. Journal of Pediatric Surgery, 47(1), 217-221.