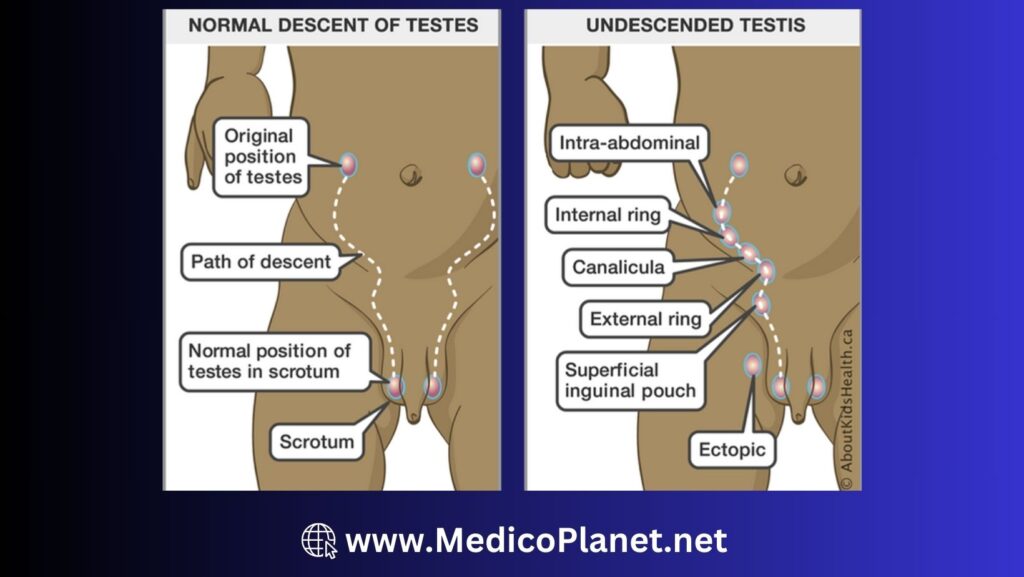
Undescended testes, or cryptorchidism, is a common congenital condition in which one or both testes fail to descend into the scrotum.
- More common in preterm infants( 25%-30%)
- Timely intervention is essential to minimize the risk of complications, including infertility and an increased risk of testicular cancer
Types:
- True undescended testes (UDT): Testes found along its normal path of descent but not reached scrotum
- Ectopic Testes: Testes found outside its normal path of descent and outside the scrotum
- Retractile Testes: Normally descended testes, found in a suprascrotal position due to an overactive cremasteric reflex
- Ascending testes or acquired undescended testes: These are usually iatrogenic.
History and examination
- Risk factors: Prematurity(25-30%), low birth weight, family history, intrauterine growth restriction
- History o fAbsence of one or both testes in the scrotum, noticed by parent
| Symptoms | Signs |
| Absence of one or both testes in the scrotum | Empty scrotum on one or both sides Inguinal or abdominal palpable testis |
Examination Tips:
- Warm your hands, put baby in supine, frog leg position with both legs free
- Observe scortum for hypoplasia
- Examine the inguinal region first before scrotum to prevent activation of cremastric reflex.
- Look for testis in normal path of descent (Abdominal, Inguinal, Suprascrotal)
- Assess testicular mobility, size, consistency, and spermatic cord tension.
- If not found, look at the ectopic location (Inguinal region, perineum, femoral canal, penopubic area)
- Don’t forget to examine the contralateral testes. Check the size, location, and texture of the contralateral descended testis. It usually have compensatory hypertrophy.
- Look for associated findings such as hernia, hydrocele, penile size, and meatal position.
How to differentiate retractile testes from undescended testes?
The retractile testis will remain intrascrotal after overstretching of the cremaster muscle, whereas a low cryptorchidic testis will return to its undescended position after being released.
Differential diagnosis (D/D) & Complication
D/D:
- Retractile testis (Testis temporarily moves out of the scrotum due to cremasteric reflex)
- Ectopic testis (Testis located outside the normal path of descent)
- Anorchia (Absence of testis)
- Disorders of sexual differentiation ( if associated with hypospadias)
Complications:
- Infertility
- Testicular torsion
- Increased risk of testicular cancer
Investigation
- Physical examination to locate the testis (inguinal, abdominal, or ectopic)
- Imaging: Ultrasound (if the testis is non-palpable); MRI (in select cases)
Note: There is no role for routine imaging in undescended testes ; Ultrasound lacks the efficacy to detect or definitively say there is no intra-abdominal testes ; Magnetic resonance imaging is rarely used in cases of disorder of sexual differentiation (DSD) to look for Müllerian structures along with the testes.
Admission criteria
- Not routinely required unless surgery is planned
Management
Undescended testes rarely descends after 6–10 months, hence orchidopexy should be performed as early as possible after 10 months of age to prevent progressive loss of germ cells. UDT can undergo torsion at any age and emergency surgery is warranted in case of acute pain with redness.
Observation: For infants younger than 6 months, as spontaneous descent may occur
Surgical:
- Surgery is planned between the 6th to the 12th month of age.
- Indication: Persistent undescended testes beyond 6 months of age
- Procedure:
- Orchidopexy (surgical relocation of the testis to the scrotum)
- For Non-palpable testes: Exploration for a non-palpable testis is usually performed with laparoscopy. Once the testes is located by laparoscopy, it may be brought down into the scrotum in a single or two stage procedure
- For palpable testis– standard open orchidopexy
- If non-palpable testis-laparoscopic assisted orchidopexy-either as single stage or two-stag
Note: Most orchidopexy operations are done as day case procedures. Children require inpatient admission if pain control is inadequate post operatively and if there are co-morbid conditions that require monitoring in the post op.
Advices
- Monitor for signs of complications, such as testicular torsion or a growing mass
- If a newborn boy has been found to have an undescended testis, the family needs to be counseled about the need for review at 6 months and the possibility of surgery. In case of pain and swelling in the groin, there is a possibility of torsion and emergency intervention is necessary
- Boys with undescended testes may suffer from lower fertility rates ; Age at intervention and laterality is an important predictive factor ; 2–8 fold increase in risk of malignancy. Close follow-up warranted after puberty
Referral
- Refer to a pediatric surgeon or pediatric urologist for evaluation and surgical management
- Child with undescended testis referred to higher centre if:
- Severe hypospadias with unilateral non palpable testis
- Nonpalpable testis with or without hypospadias
- Dysmorphic child and a syndrome suspected
Follow up
- Regular follow-up with a pediatrician or pediatric surgeon to monitor testicular position and growth
- Children are usually followed up as per the following time table:
- 1 week after surgery
- 3 months after surgery
- Annually thereafter till puberty
- Testicular self examination is taught to the boy at puberty
References
- Barthold, J. S., & Gonzalez, R. (2003). The epidemiology of congenital cryptorchidism, testicular ascent and orchiopexy. Journal of Urology, 170(6 Pt 1), 2396-2401.
- Trsinar, B., & Muravec, U. R. (2009). Fertility potential after unilateral and bilateral orchidopexy for cryptorchidism. World Journal of Urology, 27(4), 513-519.
- Kolon, T. F., Herndon, C. D., Baker, L. A., Baskin, L. S., Baxter, C. G., Cheng, E. Y., … & Meyer, T. (2014). Evaluation and treatment of cryptorchidism: AUA guideline. Journal of Urology, 192(2), 337-345.