Imperforate anus is a congenital malformation in which the rectum and anus do not properly develop, resulting in the absence of a normal anal opening. This condition occurs in approximately 1 in 5,000 live births and can be associated with other anomalies, such as VACTERL association.
VACTREL Syndrome:
- Vertebral defects – e.g., small hypoplastic vertebrae or hemivertebra
- Anal defects – anal atresia/imperforate anus
- Cardiac defects – e.g., ventricular septal defects, atrial septal defects, or tetralogy of Fallot
- Tracheoesophageal fistula
- Renal defects – Complete or partial renal genesis (either unilateral or bilateral), other genitourinary system anomalies
- Limb defects – missing or displaced digits, polydactyly, or syndactyly (i.e., webbed or fused fingers or toes)
History and examination
- Newborns, often detected shortly after birth
- Risk factors: Family history, maternal exposure to certain medications or toxins, VACTERL association
- History: Absence of anal opening, inability to pass meconium, abdominal distension
| Symptoms | Signs |
| Absence of anal opening Inability to pass meconium within 24 hours Abdominal distension | Absent or abnormally positioned anal opening Fistula between the rectum and perineum, urethra, or vagina |
Differential diagnosis (D/D) & Complication
D/D:
- Hirschsprung disease (Aganglionic colon segment, delayed meconium passage, but normal anal opening)
- Anorectal malformation (Spectrum of disorders, may include imperforate anus)
Complications:
- Infection
- Urinary and fecal incontinence
- Constipation
Investigation
- Physical examination: Assess for the presence and location of the anal opening and associated fistulas
- Imaging: Abdominal X-ray, ultrasound, and MRI to evaluate the extent of the anomaly and associated conditions
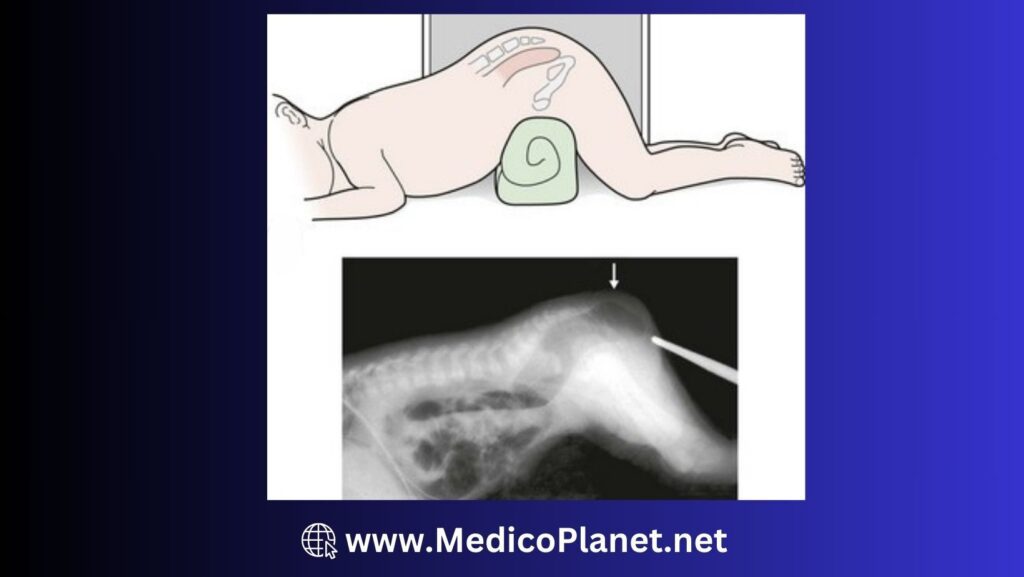
- X-ray: Lateral film radiograph in prone position should be done to determine the location of the distal bowel air bubble from the anal dimple (marked by the placement of a lead marker). A distance of less than 1 cm usually indicates a low defect, and greater than 1 cm distance may indicate a high defect.
- Echocardiogram and renal ultrasound to assess for VACTERL association
Admission criteria
- Immediate admission for infants with confirmed or suspected imperforate anus for surgical evaluation and management
Management
Emergency management:
- Nil per oral
- Nasogastric tube placement for abdominal decompression ( Keep the opening of NG tube open)
- Intravenous fluids
Medical:
- Supportive care (fluid resuscitation, electrolyte management)
- Start antibiotic (Inj Amoxicillin or Gentamycin)
Surgical:
- Indication: Confirmed diagnosis of imperforate anus
- Procedure: Staged surgical repair, including initial colostomy and definitive anorectal reconstruction (e.g., posterior sagittal anorectoplasty)
Advices
- Postoperative care includes monitoring for complications and providing support for bowel and urinary function
Referral
- Refer to a pediatric surgeon for confirmation of diagnosis and surgical management
References
- Levitt, M. A., & Peña, A. (2007). Anorectal malformations. Orphanet Journal of Rare Diseases, 2(1), 33.
- Bischoff, A., & Levitt, M. A. (2016). Congenital anorectal malformations. In Holcomb and Ashcraft’s Pediatric Surgery (6th ed., pp. 511-528). Elsevier.
- Cuschieri, A. (2001). Anorectal malformations in children: embryology, diagnosis, surgical management and prognosis. ANZ Journal of Surgery, 71(6), 361-374.